







")












Back pain is very common among women. For some women, back pain starts after delivery, and for others during the postmenopausal period. Many women live with symptoms for years before seeking help, often because they believe that pelvic pressure, urinary leakage, and a sensation of heaviness in the lower belly are simply the price of motherhood or aging.
One of the major causes of back pain is pelvic organ prolapse. While often ignored, it can affect daily routine, sleep, and overall quality of life. Pelvic organ prolapse occurs when one or more pelvic organs, such as the uterus, bladder, or rectum, descend from their normal position and bulge into the vagina.
The brighter side is that there are effective treatments from physiotherapy to surgery. Here is what it is, who it affects, and what to do about it.
- Pelvic organ prolapse happens when organs such as the bladder, uterus, or rectum slip down into the pelvic floor and bulge into the vagina.
- It is most common in women after childbirth and menopause.
- Sometimes it’s silent and found only during routine exams.
- Symptoms are heaviness in the lower tummy, urinary leakage, bowel difficulties, back pain, or discomfort during sex.
- It can be effectively managed by treatment.
What Pelvic Organ Prolapse Is — and the Different Types
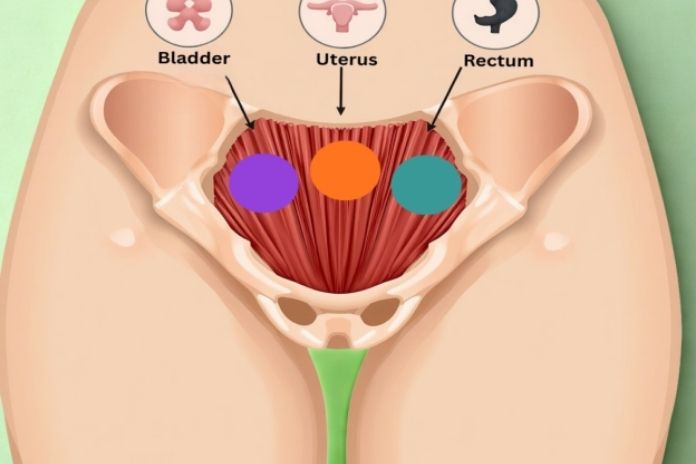
Your pelvic floor is a group of muscles in the lower hip area. These muscles act like a supportive base, holding up your bladder, uterus, and bowel, often called the pelvic organs, so they stay in place and function properly.
What Is Pelvic Organ Prolapse?
When the pelvic floor muscles become weak or are damaged, they may not be able to hold the organs as firmly as before. As a result, one or more of the pelvic organs can slip down from their usual position and create a bulge into or even through the vaginal wall. This condition is known as pelvic organ prolapse.
Think of it as the body’s support system losing some of its strength, causing the organs to shift. While it can sound worrying, understanding what’s happening is the first step toward finding relief and solutions.
Different Types of Pelvic Organ Prolapse
Pelvic organ prolapse can affect different organs, and the type is named after the organ that has shifted. They are as follows:
- Cystocele (Bladder Prolapse):This is the most common type. The bladder drops toward the front wall of the vagina, often leading to urinary symptoms such as frequent urination, leakage, or difficulty fully emptying the bladder.
- Rectocele (Rectum Prolapse):Here, the rectum bulges into the back wall of the vagina. Women may notice difficulty with bowel movements, a feeling of incomplete emptying, or pressure in the vaginal area.
- Uterine Prolapse: The uterus descends into the vaginal canal. It can range from a mild drop to a complete protrusion through the vaginal opening. Symptoms may include a heavy feeling in the pelvis, discomfort, or visible bulging.
- Vaginal Vault Prolapse: This occurs after a hysterectomy, when the top of the vagina loses support and descends. Though less common, it can be significant and cause a feeling of pressure or bulging.
- Enterocele (Small Bowel Prolapse):In this type, the small intestine pushes into the upper vaginal wall. Women may feel a sense of fullness, pressure, or discomfort, especially when standing for long periods.
Many women experience more than one type of prolapse at the same time. This is called mixed prolapse, and it’s quite common. When multiple organs are involved, the symptoms can overlap, and the treatment approach varies.
“Pelvic organ prolapse is a condition that afflicts women of all ages, and it is defined as the herniation or droppage of the internal female organs, the bladder, the uterus, or the rectum, down into the vagina at different levels of severity.”
Dr. Vatche Minassian, chief urogynecologist at Brigham and Women’s Hospital in Boston
Read More: Pelvic Floor Dropping After Childbirth: What’s Normal and What’s Not
Who Gets It — Risk Factors and Prevalence

Pelvic organ prolapse can affect women of all ages, but it’s most often seen in those who have given birth and in older women after their periods have stopped (postmenopausal).
The major risk factors are as follows:
- Vaginal Childbirth: The strongest risk factor is vaginal delivery, which places intense strain on the pelvic floor muscles and ligaments. Prolonged labor, instrumental deliveries (like forceps or vacuum), large babies, and multiple births further increase the likelihood. Even after uncomplicated deliveries, many women may have mild or “silent” prolapse that isn’t immediately noticeable.
- Menopause: It often accelerates the progression of prolapse. As estrogen levels drop, the collagen and connective tissues that support the pelvic organs become weaker. That’s why many women who had only mild or unnoticed prolapse for years begin to experience more noticeable symptoms in their 50s and 60s.
- Chronic Straining: Chronic straining, whether from constipation, heavy lifting, or a long‑term cough, puts repeated pressure inside the abdomen. Over time, this constant stress can wear down the pelvic floor muscles and gradually weaken their ability to provide support.
- Obesity: Obesity places extra weight and pressure on the pelvic floor. Over time, this added load can strain the supporting muscles and tissues, making them more vulnerable to weakening and prolapse.
- Previous Pelvic Surgery: Pelvic surgery, such as hysterectomy, alters pelvic support, and this extra pressure increases the risk for vaginal vault and enterocele prolapse.
- Connective Tissue Disorders: Connective tissue disorders can weaken the body’s collagen, making the pelvic floor less stable. Women with hypermobility syndromes or genetic collagen variants often develop prolapse earlier and with more severe symptoms.
“Pelvic organ prolapse gets more common as women age. It is more common in women who have had children, multiple children, big children,” said Dr. Vatche Minassian.
Symptoms — What Prolapse Feels Like

Pelvic organ prolapse isn’t always about noticing a bulge. In fact, many women experience symptoms that seem unrelated to the pelvic floor and don’t immediately connect them to prolapse.
The Hallmark Symptom
A common complaint is a feeling of heaviness or pressure in the pelvis, especially after prolonged standing at the end of the day. Some women describe it as “something coming down” which is typically worse at the end of the day, after prolonged standing, or after exercise.
Urinary Symptoms
Urinary symptoms of pelvic organ prolapse can vary. Some women experience stress incontinence, where urine leaks during coughing, sneezing, or exercise. Others may notice a sense of urgency, frequent trips to the bathroom, or difficulty fully emptying the bladder. In some cases, women even need to shift position to start urination.
Bowel Symptoms
Bowel symptoms of pelvic organ prolapse often include difficulty fully emptying the bowel or a lingering sense of incomplete evacuation. Some women may even need to apply gentle pressure with a finger around the vaginal area (called manual reduction) to help with bowel movements.
Sexual Symptoms
Sexual symptoms of pelvic organ prolapse can include discomfort, pain, or reduced sensation during intercourse. For some women, the physical changes or embarrassment about the prolapse may lead them to avoid sex altogether.
Lower Back Pain
Low back pain can be a symptom of pelvic organ prolapse, particularly when the uterus or the vaginal vault is involved. The added strain on pelvic support structures often radiates as discomfort in the lower back
It’s important to know that many early‑stage prolapses (Stage I–II) don’t cause any noticeable symptoms.
In these cases, the condition is often discovered by chance during a routine pelvic exam. The absence of the classic bulge doesn’t mean prolapse isn’t present or that it isn’t contributing to bladder or bowel problems. Even without visible changes, altered pelvic floor support can interfere with normal urinary or bowel function.
Read More: What is a Prolapsed Bladder? Symptoms Women Shouldn’t Ignore
Diagnosis — What to Expect
Pelvic organ prolapse is usually diagnosed through a clinical pelvic examination. In most cases, no imaging is required. A general practitioner (GP) can perform the initial assessment, but if symptoms are present or treatment decisions are required, referral to a urogynecologist or gynecologist is appropriate.
The POP‑Q (Pelvic Organ Prolapse Quantification) system is the international gold standard for staging. It measures how far each vaginal wall compartment descends in relation to the vaginal opening, recorded in centimeters. For example, Stage II prolapse reaches the level of the hymen, while Stage III extends beyond it.
When urinary symptoms are significant, urodynamic testing may be added to evaluate bladder function before surgery is considered. MRI scans are reserved for complex or unusual cases where more detailed imaging is necessary.
Read More: Breathing Techniques for Pelvic Floor Relaxation and Strength: A Guide to Core-Connected Calm
Treatment Options — From Physiotherapy to Surgery

Treatment is tailored to the severity of symptoms, type of prolapse, and personal preferences. Surgery is not always the first step; many women benefit from conservative approaches.
Pelvic Floor Muscle Training (PFMT)
- Considered the first‑line treatment for Stage I–II prolapse.
- A Cochrane review confirms PFMT can reduce symptoms and even lessen the degree of prolapse.
- Physiotherapist‑led programs consistently outperform self‑directed exercise, making referral to a pelvic floor physiotherapist appropriate for most women.
Pessary
- A removable silicone device placed in the vagina to support prolapsed organs.
- Ring pessaries are most commonly used.
- Effective at all stages, reversible, and suitable for women who wish to avoid surgery, are pregnant, or have medical reasons to delay surgery.
- After initial fitting, most women can self‑manage pessary care.
Lifestyle Modifications
- Weight loss to reduce pelvic pressure.
- Managing constipation to avoid straining.
- Stopping smoking to reduce chronic cough.
- Avoiding heavy lifting to minimize mechanical stress on the pelvic floor.
Topical Vaginal Estrogen
- Topical vaginal estrogen is usually applied directly inside the vagina.
- In postmenopausal women, local estrogen improves vaginal tissue quality and enhances the effectiveness of other treatments.
- Local hormone therapy works only in the area it’s applied, so it doesn’t affect the whole body. That means it can still be used safely even if full‑body (systemic HRT) hormone therapy isn’t suitable for you.
Surgery
Surgery is usually considered when conservative treatments don’t provide enough relief or when the prolapse is more advanced (Stage III–IV). Surgical repair can be very effective, often improving bladder, bowel, and pain symptoms.
Common Surgical Options
- Vaginal wall repair (anterior/posterior colporrhaphy): Strengthens the vaginal walls.
- Sacrospinous ligament fixation: Uses strong ligaments to support the upper part of the vagina.
- Sacrocolpopexy (Laparoscopic or robotic): A minimally invasive procedure that lifts and secures the upper part of the vagina using mesh.
The choice of surgery depends on the type of prolapse, its severity, and individual health factors.
When to See a Doctor

You should book an appointment with your GP if you notice:
- A new or worsening feeling of pelvic heaviness or pressure
- A bulge or fullness at the vaginal opening
- Urinary problems such as leakage, urgency, or difficulty emptying the bladder without another clear cause
- Bowel difficulties, like trouble emptying
- Discomfort during sex
Pelvic organ prolapse does not go away on its own, but it can be well managed with the right treatment. Getting checked early means doctors can often offer more conservative options and help ease symptoms before they progress.
Final Thoughts

Pelvic organ prolapse is common, often under‑reported, yet highly treatable.
The gap between how many women experience it and how many seek help often comes from normalization—the belief that pelvic heaviness, leakage, or pressure are simply the price of childbirth or aging. These are consequences, not life sentences.
Effective treatments exist at every stage, from pelvic floor physiotherapy to pessary use to surgery. The most important step is acknowledging the condition; solutions can follow from there.
FAQs
1. Is pelvic organ prolapse serious?
Pelvic organ prolapse is rarely dangerous; it does not turn cancerous or spread to other parts of the body. However, it can cause symptoms such as pelvic pressure, a feeling of fullness, and changes in bladder or bowel function.
These issues may not threaten life, but they can significantly affect comfort and daily routines if left untreated. The seriousness lies in its impact on quality of life: prolapse often worsens over time, and earlier treatment is usually more effective and less invasive than waiting until symptoms become severe.
2. Can pelvic organ prolapse be fixed without surgery?
Yes. Pelvic organ prolapse can often be managed without surgery. Pelvic floor muscle training is especially effective in reducing symptoms and improving prolapse in early stages (Stage I–II). Vaginal pessaries, which provide mechanical support, can be used at any stage and are a safe long‑term option for many women.
Lifestyle changes, such as maintaining a healthy weight and avoiding heavy lifting, also help slow progression. Surgery is usually considered only when conservative measures no longer control symptoms, or in advanced cases (Stage III–IV) that significantly affect daily life. Many women successfully choose pessary management as a long‑term alternative to surgery.
3. Can pelvic floor exercises reverse prolapse?
Pelvic floor muscle training (PFMT) can ease symptoms and reduce the severity of prolapse, especially in its early stages. While exercises are unlikely to fully reverse advanced prolapse (Stage III–IV), they can still improve comfort and slow progression.
Starting pelvic floor training before and after childbirth offers the best preventive benefit, helping women strengthen support structures and reduce future risk. In short, PFMT is a safe, proven strategy for managing prolapse and protecting pelvic health.
4. Does prolapse affect sex?
Prolapse can affect sex. Many women experience discomfort during intercourse, reduced sensation, or may avoid intimacy due to embarrassment or anxiety. Managing prolapse through pelvic floor exercises, pessary use, or surgery often improves sexual function. In postmenopausal women, topical estrogen can also enhance tissue quality and comfort, making intimacy better.
References
- Kuo, C.-H., Martingano, D. J., & Mikes, B. A. (2024). Pelvic organ prolapse. StatPearls Publishing.
- Cleveland Clinic. (2024, December 4). Pelvic organ prolapse: Types, causes & treatment.
- Badiu, D., Onuc, S., Niculescu, C., Delcea, C., & Tica, V. (2025). Pelvic organ prolapse after vaginal birth: A qualitative study on treatment perspectives.
- Cleveland Clinic. (2024, December 4). Pelvic organ prolapse: Types, causes & treatment.
- Woodley, S. J., Boyle, R., Cody, J. D., Mørkved, S., & Hay‑Smith, E. J. C. (2020). Pelvic floor muscle training for prevention and treatment of urinary and faecal incontinence in antenatal and postnatal women.
- Chung, S.-H., & Kim, W. B. (2018). Various approaches and treatments for pelvic organ prolapse in women. Journal of Menopausal Medicine.
In this Article