











")









Ear pressure is something most people experience at some point, after a cold, during a flight, or while driving through changing altitudes. In most cases, it resolves within hours. You swallow, yawn, or hear a small pop, and everything returns to normal.
But when that pressure lingers for days or even weeks, when the ear feels constantly clogged, hearing becomes muffled, and nothing seems to relieve it, it may no longer be simple congestion. Persistent symptoms often point to a deeper issue with how the ear is regulating pressure. This is where the eustachian tube dysfunction comes in. When it fails to open properly, pressure builds up inside the middle ear.
Over time, this creates negative pressure that can pull the eardrum inward, leading to a condition called eardrum retraction (also known as tympanic membrane retraction or middle ear atelectasis). It tends to develop gradually, which is why it’s often overlooked in the early stages.
While it may seem minor at first, untreated eardrum retraction can lead to structural changes and more serious complications. Understanding what’s happening, recognizing the warning signs, and seeking timely evaluation can make a significant difference in preventing long-term damage.
- Persistent ear pressure after a cold, allergy, or flight often points to eustachian tube dysfunction. This means the ear can’t equalize pressure properly.
- Key signs include fullness, muffled hearing, crackling sounds, and a pulling sensation. Symptoms often return after every illness or altitude change.
- If these symptoms persist, it’s not just a temporary clog. An ENT evaluation is needed to prevent long-term damage.
Read More: Can Holding in a Sneeze Damage Your Brain or Ears? What Doctors Say
What It Means When the Eardrum “Collapses” or Retracts
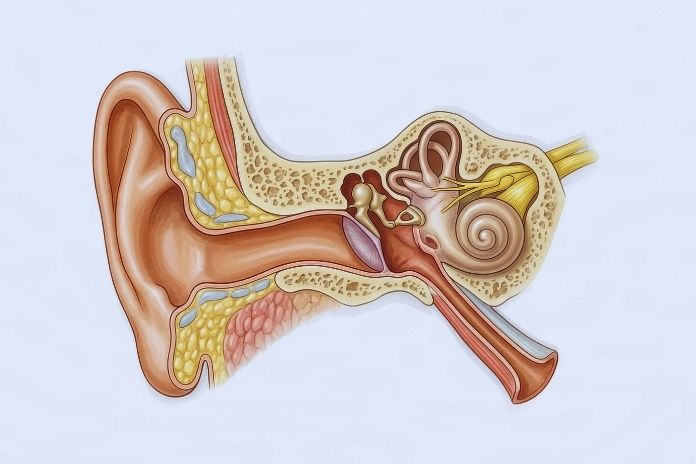
The eardrum, or tympanic membrane, is a thin membrane stretched across the ear canal that separates the outer ear from the middle ear. For it to vibrate correctly and transmit sound, the air pressure on both sides must be roughly equal.
That equilibrium is maintained by the eustachian tube, a narrow canal about 3.5 centimeters long in adults that connects the middle ear to the back of the nasopharynx. The eustachian tube is normally closed. It opens briefly each time you swallow, yawn, or chew, allowing a small amount of air to flow into the middle ear and equalizing any pressure difference that has built up.
Most people do this dozens of times an hour without ever noticing it. When the tube functions normally, the tympanic membrane sits in a neutral position: neither bulging outward nor retracting inward.
What Causes the Eardrum to Pull Inward
Eardrum retraction begins when the eustachian tube is blocked or inflamed and cannot open to allow air in. The mucosa of the middle ear gradually absorbs the trapped air, creating a progressively lower air pressure environment on the inner side of the eardrum. The higher atmospheric pressure on the outer side then pushes the eardrum inward.
In mild cases, the eardrum simply appears to be in a retracted position on examination. In more advanced cases, it is pulled into contact with the ossicles, the small hearing bones of the middle ear, or is drawn into pockets that can develop into structural problems over time.
A 2006 review published in the Otolaryngologic Clinics of North America classified middle ear atelectasis into four grades based on the severity of tympanic membrane retraction, from mild inward displacement to full adherence of the eardrum to the middle ear wall. The classification is clinically useful because the grade determines urgency and treatment approach.
Why Retraction Can Progress Over Time
The eardrum is not a rigid structure. It is a flexible membrane that responds to sustained pressure gradients by deforming. If eustachian tube dysfunction symptoms persist without resolution, the eardrum can develop retraction pockets, particularly in the pars flaccida, the more elastic upper portion of the eardrum.
These pockets are clinically significant because they can accumulate debris and skin cells, creating conditions for cholesteatoma formation, an abnormal growth that can erode surrounding bone if it progresses unchecked.
5 Signs Ear Pressure May Be More Than a Temporary Clog

1. Persistent Ear Fullness That Doesn’t Improve With Popping or Swallowing
The most consistent symptom of eardrum retraction and sustained eustachian tube dysfunction is ear fullness that does not respond to the usual equalizing maneuvers. Normal pressure changes from altitude or congestion resolve within hours.
Ear pressure not going away after 48 to 72 hours, particularly in someone who has recently had a respiratory illness or allergic episode, is the clearest early signal that the eustachian tube is not clearing the pressure differential on its own. The ear may feel as though it is packed with cotton, submerged in water, or blocked by something that cannot be dislodged.
A multidisciplinary international consensus statement identified persistent aural fullness, pressure, and inability to equalize middle-ear pressure as hallmark symptoms of Eustachian tube dysfunction, particularly when symptoms are chronic or recurrent.
2. Muffled Hearing or Sudden Changes in Sound Clarity
Conductive hearing loss is one of the direct consequences of tympanic membrane retraction. When the eardrum is pulled inward, it cannot vibrate with its normal mechanical efficiency. Sound transmission through the middle ear is reduced, and the result is a muffled, slightly dampened quality to all sounds.
Music sounds flat. Speech sounds as though it is coming from a distance. High-pitched sounds may disappear entirely or become difficult to localize. This type of hearing change is distinct from sensorineural hearing loss in that it reflects a mechanical problem in the conduction pathway rather than damage to the inner ear or auditory nerve.
A 2017 study examined eustachian tube function in patients with tympanic membrane retraction compared to normal subjects and found that reduced eustachian tube functional efficiency was the dominant variable predicting the degree of retraction, with greater tube dysfunction associated with worse conductive hearing loss outcomes.
3. Clicking, Crackling, or Popping Sounds Inside the Ear
Chronic ear pressure often produces audible mechanical sounds as the eustachian tube intermittently attempts to open against a negative pressure gradient. Clicking when swallowing, crackling during jaw movement, or a single pop that brings brief relief before pressure returns are all characteristic of eustachian tube dysfunction symptoms.
These sounds reflect the tube struggling to equalize a pressure differential that has built up beyond what normal tube opening can quickly correct. The sounds may be more noticeable in quiet environments, during eating, or immediately after lying down.
4. Mild Ear Pain or a Pulling Sensation
As negative ear pressure symptoms intensify and the tympanic membrane is drawn inward, the eardrum puts tension on its attachments to surrounding structures, including the malleus, the first of the three ossicles. This tension can produce a dull ache, a feeling of fullness that transitions to pressure, or a distinct pulling sensation deep in the ear canal.
The pain is typically not sharp or severe in early eardrum retraction, distinguishing it from acute otitis media. It tends to be positional or activity-related, worsening with altitude changes, air travel, or sustained jaw use.
5. Frequent Ear Pressure After Colds, Allergies, or Flights
A recurrent blocked ear that won’t pop following each upper respiratory infection or allergic episode is one of the most clinically predictive patterns for underlying eustachian tube dysfunction. Most people with healthy eustachian tube function recover ear pressure normalization within 24 to 48 hours of illness resolution.
People with structural or inflammatory tube dysfunction do not. If you find yourself dealing with ear pressure not going away after each cold, each seasonal allergy flare, or each air travel experience, that pattern is clinically meaningful and worth discussing with an ENT even in the absence of other symptoms.
Read More: 7 Signs Your Eardrum is Ruptured
Why Eustachian Tube Dysfunction Often Triggers Eardrum Retraction

The eustachian tube’s pressure-equalizing function depends on its ability to open against a small amount of resistance each time the tensor veli palatini muscle contracts during swallowing. In healthy adults, this happens smoothly and frequently.
In eustachian tube dysfunction, the tube either fails to open fully, opens against abnormally high resistance from surrounding mucosal swelling, or is structurally compromised by anatomical factors.
Dr. Eric Smouha, MD, FACS, emphasizes the central role of the Valsalva maneuver in both assessment and conservative management: “I think that the Valsalva maneuver is really an essential part of the physical exam in these patients and helps determine the degree of severity,” he told ENTtoday.
Common Causes of Tube Blockage
The most common drivers of eustachian tube dysfunction symptoms are upper respiratory infections, allergic rhinitis, sinus inflammation, and enlarged adenoids in children. Each produces mucosal swelling that narrows or occludes the tube opening.
The relationship between allergy and tube dysfunction is particularly important because it is chronic, recurring, and often undertreated.
Why Some People Develop Chronic Ear Pressure Problems
Anatomical factors, including the angle and length of the eustachian tube, the compliance of surrounding mucosal tissue, and the function of the tensor veli palatini muscle, all influence susceptibility to chronic eustachian tube dysfunction.
Children are significantly more vulnerable because their tubes are shorter, more horizontal, and more easily blocked. Adults who develop chronic eardrum retraction often have a combination of anatomical predisposition and a persistent inflammatory trigger such as untreated allergic rhinitis or recurring sinus infections.
Possible Complications if Eardrum Retraction Persists

When tympanic membrane retraction is sustained, and the eustachian tube remains dysfunctional, the middle ear mucosa responds to the negative pressure environment by producing fluid.
Otitis media with effusion, commonly called glue ear, develops when this fluid accumulates without infection. The fluid further impairs eardrum mobility, worsening conductive hearing loss and creating a middle ear environment that is more susceptible to secondary bacterial infection.
Conductive Hearing Loss
Conductive hearing loss from eardrum retraction ranges from mild to moderate, depending on the degree of retraction and whether fluid is present. When the eardrum is pulled into contact with the ossicles, the mechanical coupling of the hearing chain is disrupted.
Long-standing retraction that produces adhesions between the eardrum and middle ear structures can produce more significant hearing loss that does not fully resolve even after the underlying pressure problem is corrected.
Structural Changes in the Eardrum
A 2010 Cochrane review examining surgery for tympanic membrane retraction pockets noted that untreated retraction pockets can progress to cholesteatoma formation, in which squamous epithelium accumulates in the retraction pocket and begins to erode surrounding bone.
Cholesteatoma is a serious complication that requires surgical management and represents the most significant long-term risk of unmonitored eardrum retraction in vulnerable patients.
How Doctors Diagnose a Retracted Eardrum

Physical Ear Examination With an Otoscope
The first step in diagnosing retracted eardrum symptoms is direct visualization through an otoscope. An experienced clinician can identify the characteristic appearance of a retracted eardrum, including altered light reflex, increased visibility of the ossicular landmarks, and visible retraction pockets in the pars flaccida.
The degree of retraction visible on otoscopy helps guide the urgency of further testing.
Tympanometry to Measure Ear Pressure
The tympanometry test is the most objective bedside measure of middle ear pressure and eardrum compliance. A small probe placed at the ear canal entrance varies the air pressure while measuring the eardrum movement.
In eardrum retraction caused by eustachian tube dysfunction, the tympanogram typically shows a type C pattern, indicating negative middle ear pressure, or a type B pattern if fluid is present. A normal type A tympanogram effectively rules out significant retraction or effusion.
Dr. Seilesh Babu, MD, emphasizes that thorough evaluation includes direct assessment of tympanic membrane retraction alongside audiogram and nasopharyngoscopy: his clinical approach to patients with persistent ear pressure not going away systematically evaluates for retraction, middle ear fluid, and eustachian tube movement before any intervention is considered.
Hearing Tests if Hearing Changes Are Present
A formal audiogram confirms the type and degree of hearing loss. In eardrum retraction, the audiogram typically shows a conductive pattern with an air-bone gap, meaning bone conduction is normal, but air conduction is reduced.
This pattern confirms that the problem is in the conductive pathway rather than the inner ear and helps distinguish eardrum retraction from sensorineural causes of muffled hearing.
Treatment Options for Persistent Ear Pressure

Because eustachian tube dysfunction driving eardrum retraction is most commonly caused or aggravated by nasal and sinus inflammation, treatment typically begins with the upper airway. Intranasal corticosteroid sprays reduce mucosal swelling at the tube opening.
Antihistamines and allergy immunotherapy address the underlying allergic trigger in patients with confirmed allergic rhinitis. Sinus disease management with saline irrigation and antibiotics, where indicated, reduces the inflammatory load on the eustachian tube opening.
The Valsalva maneuver, performed by gently blowing against pinched nostrils with the mouth closed, can temporarily open the eustachian tube and equalize pressure. The Toynbee maneuver, swallowing while the nose is pinched, and the Frenzel maneuver, using tongue pressure to push air up the tube, are alternatives that some patients find more comfortable.
Nasal balloon devices such as the Otovent, which uses nasal exhalation to inflate a balloon and deliver pressure to the Eustachian tube opening, have evidence of benefit in children with middle ear ventilation problems and are increasingly used in adults.
Dr. Michael Harris, MD, ENT surgeon at Sleep and Sinus Centers of Georgia, describes the impact of newer procedural options for chronic cases: “Balloon dilation has transformed treatment of chronic ETD.
Evidence from a randomized controlled trial found that balloon dilation significantly improved symptoms and objective measures of Eustachian tube function compared with continued medical therapy alone in adults with persistent ETD.
Many patients experience relief within days and report a better quality of life,” he notes, identifying balloon eustachian tube dilation as a significant development for patients who have not responded to conservative management.
When conservative measures fail, ventilation tube insertion through the eardrum, a myringotomy, provides immediate pressure equalization by bypassing the dysfunctional eustachian tube. The tube allows air into the middle ear directly, resolving the negative-pressure environment that drives retraction.
In advanced tympanic membrane retraction with retraction pockets or early cholesteatoma, surgical management may be needed to remove the pocket and reconstruct the eardrum.
When Ear Pressure Should Be Evaluated by a Doctor
Symptoms lasting more than a few weeks without improvement, including the ear feeling clogged but no wax on examination, are the primary threshold for ENT evaluation. Conductive hearing loss that persists beyond the resolution of a cold, negative ear pressure symptoms that recur with each illness or altitude change, and ear discomfort accompanied by clicking or crackling all warrant assessment rather than continued watchful waiting.
Symptoms occurring after head trauma, a sudden pressure event such as a very hard nose blow, or underwater diving should be evaluated more urgently to rule out perilymph fistula or other acute structural injury. Any eardrum retraction accompanied by drainage from the ear, bleeding, or neurological symptoms is a red flag requiring prompt evaluation.
Read More: Safe and Effective Methods To Keep Your Ears Clean
Key Takeaway
Persistent ear pressure isn’t always a lingering cold. When it doesn’t improve and is paired with muffled hearing, clicking, or difficulty equalizing, it often points to eustachian tube dysfunction, where negative pressure begins pulling the eardrum inward. This leads to eardrum retraction, a structural change that is easier to manage early but more complex if delayed.
Diagnosis is straightforward with tympanometry and otoscopy, and treatment ranges from medications to minor procedures depending on severity. Catching retracted eardrum symptoms early helps protect hearing and prevents long-term damage to the middle ear.
Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. Consult a qualified ENT specialist or healthcare provider regarding any symptoms of ear pressure, hearing changes, or ear discomfort.
References
- Babu, S. (2024). Myringotomy for eustachian tube dysfunction. BackTable ENT Podcast.
- Canali, I., et al. (2017). Assessment of eustachian tube function in patients with tympanic membrane retraction. Brazilian Journal of Otorhinolaryngology, 83(4), 381-387.
- Danner, C. J. (2006). Middle ear atelectasis: What causes it and how is it corrected? Otolaryngologic Clinics of North America, 39(6), 1211-1219.
- Derebery, M. J., et al. (2001). Eustachian tube dysfunction as a cause of chronic ear disease in patients with allergy. Otolaryngology-Head and Neck Surgery.
- Harris, M. (2026). Eustachian tube dysfunction: Symptoms, causes, and effective treatment options. Sleep and Sinus Centers of Georgia.
- Nankivell, P. C., & Hartley, B. E. J. (2010). Surgery for tympanic membrane retraction pockets. Cochrane Database of Systematic Reviews.
- Smouha, E. (2018). Eustachian tube dysfunction: Panel discussion on aural fullness and Valsalva. ENTtoday.
- Urík, M., Tedla, M., & Hurník, P. (2021). Pathogenesis of retraction pocket of the tympanic membrane: A narrative review. Medicina, 57(5), 425.
- Washington State Health Care Authority. (2015). Tympanostomy tubes in children: Final evidence report.
- National Technical Information Service. (n.d.). Underlying eardrum perforations. Science.gov.
- American Academy of Otolaryngology–Head and Neck Surgery Foundation. (n.d.). Resident manual of trauma to the face, head, and neck.
- Department of Occupational Safety and Health Malaysia. (2024). Guidelines on management of occupational noise-related hearing disorders.
- Saudi Journal of Occupational Health. (2004). 5th International Conference of the Saudi Occupational Health Society.
In this Article


