







")








Malaria remains one of the most devastating infectious diseases affecting children across the globe, particularly in tropical and subtropical regions of Africa, Asia, and Latin America. It is not just a medical challenge but a public health emergency that disproportionately affects the most vulnerable: children under five years of age.
According to the World Health Organization (WHO), an estimated 247 million cases of malaria were reported globally in 2022, leading to more than 619,000 deaths. Tragically, over 76% of these deaths occurred in children under five, highlighting the urgent need for awareness, prevention, and timely care.
This isn’t just a statistic, it’s a call to action.
For parents and caregivers, knowledge is power. Often, you are the first line of defense. Recognizing malaria’s early symptoms, understanding how it is transmitted, knowing when and where to seek help, and implementing effective prevention strategies can be the difference between life and death.
This guide is designed to empower you. It breaks down everything you need to know about malaria in children—from identifying early signs and getting a prompt diagnosis to choosing the right treatment and adopting powerful, proven prevention measures. With the right information, you can act quickly, protect your child, and help reduce the toll malaria takes on families and communities worldwide.
What Causes Malaria in Children?

Malaria is caused by Plasmodium parasites, microscopic organisms that infect and destroy red blood cells. Of the five species known to infect humans, Plasmodium falciparum is the most dangerous, responsible for the vast majority of severe cases and deaths, especially in children. These parasites are transmitted through the bites of infected female Anopheles mosquitoes, which typically feed at night, between dusk and dawn.
While anyone can contract malaria, young children under the age of five are at the highest risk, both of getting infected and of experiencing severe, potentially fatal complications.
This increased vulnerability is due to several biological and developmental factors:
- Immature Immune Systems: Infants and toddlers haven’t don’t yet have strong immune defenses, which means their bodies are less equipped to fight off the parasite effectively.
- Rapid Fluid Loss: Symptoms like high fever, vomiting, and diarrhea can lead to severe dehydration more quickly in children than in adults, increasing the danger of rapid deterioration.
- Delayed Symptom Recognition: Young children, especially infants, often cannot articulate what they are feeling. As a result, symptoms like chills, body aches, or fatigue may go unnoticed or be mistaken for more common childhood illnesses.
Mosquitoes carrying malaria are found predominantly in sub-Saharan Africa, Southeast Asia, parts of Latin America, and the Indian subcontinent. However, even children traveling to these regions from non-endemic areas are at risk due to a lack of immunity.
Dr. Shreya Dubey, Consultant Neonatology and Pediatrics at CK Birla Hospital Gurugram, emphasizes that malaria remains a significant threat to pediatric health, particularly in tropical regions. She highlights that children under the age of five are among the most vulnerable, accounting for a large proportion of malaria-related deaths globally.
Early Symptoms of Malaria in Children

One of the most dangerous aspects of malaria in children is how easily it can be mistaken for other common illnesses, like the flu, a viral fever, or a stomach infection. In its early stages, malaria often presents with non-specific symptoms, which can delay diagnosis and treatment if proper testing isn’t done.
Common Early Symptoms
- Sudden high fever – often above 101°F (38.5°C), sometimes appearing in cycles
- Chills and shivering, typically followed by intense sweating
- Fatigue or weakness, even after adequate rest
- Irritability or persistent crying in infants and toddlers
- Loss of appetite and general discomfort
- Vomiting and/or diarrhea, which may be mistaken for a stomach bug
- Cough or rapid breathing, especially in younger children
These early signs can appear within 10–15 days of being bitten by an infected mosquito. However, in some cases, symptoms may be delayed, particularly in children who have taken partial prophylaxis or come from semi-immune regions.
If not treated promptly, malaria can progress quickly, within hours or days, into a more severe, life-threatening condition.
Severe Warning Signs Include
- Seizures or convulsions
- Pale skin or jaundice (yellowing of the eyes/skin) due to severe anemia
- Shortness of breath or labored breathing
- Confusion, drowsiness, or loss of consciousness
- Dark-colored urine, which can signal red blood cell destruction (hemolysis)
A 2021 study published in The Lancet Global Health found that delayed recognition of severe symptoms—especially in rural or resource-limited areas—was strongly linked to higher fatality rates in children under five.
Because childrens’ health can deteriorate fast, any unexplained fever in a malaria-endemic area should be tested for malaria immediately. Early detection and timely treatment save lives.
How Malaria is Diagnosed in Children
In regions where malaria is common, any fever in a child—no matter how mild—should prompt immediate testing. This is crucial because early symptoms of malaria often mimic other common illnesses, and timely diagnosis can be lifesaving. Two Key Diagnostic Methods:
Rapid Diagnostic Test (RDT)
This is a quick, simple blood test done using a small finger prick. It works by detecting malaria-specific antigens in the blood. Results are usually available within 15 to 20 minutes. RDTs are especially useful in rural or low-resource areas where laboratory facilities may not be available. However, they may not always show how many parasites are present or identify the specific Plasmodium species causing the infection.
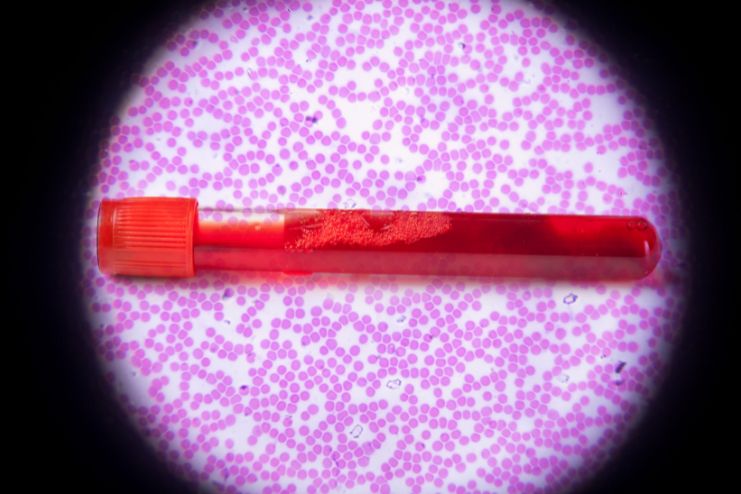
Microscopy (Blood Smear)
Considered the gold standard for malaria diagnosis, this test involves preparing a blood smear and examining it under a microscope. It confirms not just the presence of malaria but also the specific species involved and the parasite density. This information is crucial for deciding which drug to use and how long the treatment should last. Microscopy requires trained technicians and proper equipment, but it provides more detailed information than an RDT.
Treatment for Malaria in Children

Malaria in children can range from mild to life-threatening and requires careful attention. Treatment depends on several factors, including the type of malaria parasite, severity of illness, the child’s age and weight, and local drug resistance.
Both uncomplicated and severe forms need different protocols, and each step of care plays a vital role in recovery. Parents and caregivers must be informed and involved at every stage of the child’s treatment.
1. Uncomplicated Malaria
Uncomplicated malaria is the more common and less severe form. It can usually be managed at home with oral medication under proper guidance. The goal is to completely eliminate the parasite while preventing resistance or recurrence.
Treatment involves:
- Use of Artemisinin-based Combination Therapy (ACT).
- Common ACTs: Artemether-lumefantrine, Dihydroartemisinin-piperaquine, Artesunate-amodiaquine.
- Dosing is based strictly on body weight, not age.
- Complete the 3-day course even if symptoms improve early.
- Regular follow-up to monitor for possible recurrence.
2. Severe Malaria
Severe malaria is a medical emergency and must be treated in a hospital. Symptoms progress quickly, especially in young children, and can lead to organ failure or death without urgent care. Early hospitalization and intensive support improve survival outcomes significantly.
Treatment protocol includes:
- Immediate administration of intravenous artesunate for at least 24 hours.
- Full course of oral ACT once the child can tolerate medicines.
- Supportive care, like oxygen, fluids, and seizure control.
- Blood transfusions are required if severe anemia is detected.
- Continuous monitoring for signs of recovery or complications.
Read More: 17 Potent Natural Remedies to Treat Malaria and its Associated Symptoms
Prevention Tips for Parents

Preventing malaria is just as important as treating it. Simple, consistent habits at home and while traveling can make a major difference. Parents should stay proactive, informed, and consistent with these measures.
1. Use Insecticide-Treated Bed Nets (ITNs)
Sleeping under treated nets is one of the easiest and most effective ways to prevent malaria. Nets create a barrier and kill mosquitoes that come into contact. Children should use them every single night.
Key practices:
- Use long-lasting insecticidal nets (LLINs)
- Replace or re-treat nets every 3–5 years
- Ensure proper tucking around the mattress
- Use consistently during high-risk seasons
- Repair or replace torn nets immediately
According to the CDC Malaria Program, community-wide trials conducted in several African regions showed that insecticide-treated nets reduced mortality among children under five by approximately 20 percent.
2. Wear Protective Clothing and Use Repellents
Clothing and repellents create a personal shield from mosquito bites. These are especially important during early mornings and evenings when mosquitoes are most active. Safe repellent use is essential for children’s health.
Tips to follow:
- Dress children in long sleeves and pants.
- Use DEET-based repellents for kids above 2 months.
- Apply only to exposed skin, not under clothing.
- Avoid contact with eyes, mouth, or hands.
- Reapply as instructed, especially after sweating.
3. Improve Indoor Protection
Mosquito-proofing the home can drastically reduce the number of bites. Proper ventilation and targeted spraying keep living areas safe. Use physical and chemical barriers together for the best results.
Indoor strategies:
- Install fine mesh on windows and doors.
- Use WHO-approved indoor residual sprays.
- Avoid open windows at night without screens.
- Do not use mosquito coils near infants.
- Ensure cross-ventilation if any fumigants are used.
4. Preventive Medication for Travel
Children traveling to malaria-prone areas need preventive medicines. These reduce the chances of infection in children with no prior immunity. Start the medicines before travel and continue as prescribed.
Travel medication advice:
- Consult a doctor before the trip for tailored advice
- Use atovaquone-proguanil for kids over 5 kg
- Consider mefloquine for longer stays
- Doxycycline can be used for children above 8 years
- Adhere strictly to the dosage schedule before, during, and after travel
When to See a Doctor Immediately
Malaria in children can escalate within hours. Immediate medical attention is critical if your child shows:
- Any fever, especially after visiting or living in a malaria-endemic area
- Lethargy, weakness, or refusal to eat or drink
- Difficulty breathing, rapid breathing, or coughing
- Seizures or convulsions
- Severe vomiting or diarrhea
- Dark urine, yellow eyes, or very pale skin (signs of anemia or hemolysis)
- Bulging or sunken fontanelle (soft spot) in infants
Even if a child has been treated for malaria before, recurring fever can signal reinfection or drug resistance. Prompt re-testing is necessary.
Long-Term Effects and Recovery
While most children recover completely from malaria with timely treatment, some may experience lingering health issues. These are more common after severe cases or when treatment is delayed. Recovery support plays a key role in helping children regain full physical and cognitive function.
Possible long-term complications:
- Severe anemia may need blood transfusions
- Cerebral malaria can affect brain function
- Developmental delays in speech or motor skills
- Learning difficulties that persist after recovery
- Behavioral changes, such as poor attention or memory
A PubMed study found that 26% of children who survived cerebral malaria showed cognitive deficits six months after discharge.
Supportive steps during recovery:
- Schedule follow-up tests to confirm parasites are cleared
- Provide iron-rich and nutrient-dense meals
- Monitor the child’s growth and behavior over time
- Seek medical advice if learning delays or weakness persist
- Encourage gentle physical activity and mental stimulation
Conclusion
Malaria in children is not just a medical issue but a public health challenge that demands vigilance, awareness, and action.
Treatment protocols, whether for uncomplicated or severe cases, are effective when followed correctly and completely. Parents and caregivers must ensure that children receive the full course of prescribed medication, attend follow-up checks, and are monitored for any lingering symptoms or developmental concerns. Recovery does not end with a negative test—ongoing support, nutrition, and care are just as important.
Simple preventive measures remain the strongest line of defense. Protecting one child from malaria is a step toward protecting entire communities. With the right knowledge and commitment, we can break the cycle of malaria and give every child the healthy future they deserve.
References
- https://my.clevelandclinic.org/health/diseases/15014-malaria
- https://pmc.ncbi.nlm.nih.gov/articles/PMC3507524/
- https://emedicine.medscape.com/article/998942-overview
- https://kidshealth.org/en/parents/malaria.html
- http://www.medparkhospital.com/en-US/disease-and-treatment/malaria
- https://www.mayoclinic.org/diseases-conditions/malaria/symptoms-causes/syc-20351184
- https://kidshealth.org/en/parents/malaria.html
- https://www.medparkhospital.com/en-US/disease-and-treatment/malaria
- https://pmc.ncbi.nlm.nih.gov/articles/PMC3507524/
- https://www.cdc.gov/malaria/hcp/clinical-guidance/treatment-uncomplicated.html
- https://emedicine.medscape.com/article/998942-treatment
- https://www.indianpediatrics.net/sep2008/sep-731-735.htm
- https://motherlandhospital.com/consultation-when-do-you-need-to-see-a-doctor
In this Article

