







")








Most people picture catatonia as someone frozen in place, staring blankly and unreachable, because that’s the version movies tend to highlight. Real catatonia is more varied. It can involve stillness, but it can also include agitation or repetitive gestures. Some people hold unusual postures for long stretches. Others move suddenly or unpredictably.
Families often describe the person as “there but not there,” unsure what exactly they’re witnessing. Speech may fade, eye contact may drop, or movements may become slow and rigid. On the flip side, some individuals pace rapidly or repeat motions without explanation. These mixed signals make catatonia confusing. It rarely looks the same in two people.
Here’s the thing: catatonia isn’t rare, and it’s not something to wait out. It can appear in depression, bipolar disorder, schizophrenia, autism, and certain medical illnesses. Delayed treatment raises the risk of dehydration, malnutrition, and muscle complications. Early recognition matters. Most people improve quickly when the right steps are taken.
This article walks you through the essentials in a straightforward way. What catatonia is, why it develops, and how specialists diagnose it. You’ll see how symptoms are assessed and which patterns clinicians look for. We’ll also break down the treatments that work best today. The goal is clarity, not fear.
What is Catatonia? Understanding the Basics
Catatonia is best understood as a neuropsychiatric syndrome that affects movement, behavior, and responsiveness. It isn’t a disease on its own, but a sign that something in the brain’s motor and regulatory systems is off. When these circuits misfire, people may struggle to initiate movement or, in some cases, may move excessively.
That’s why the condition can look still and rigid in one person, yet restless in another. It’s a spectrum, not a single presentation. In medical literature, you’ll often see catatonia described as psychomotor dysregulation. That simply means the systems that coordinate voluntary movement and inhibition aren’t functioning normally.
This dysregulation shapes how a person sits, walks, speaks, or reacts to the world around them. For clinicians, these movement changes are key clues. They’re often more reliable than mood or thought symptoms when identifying catatonia. The old idea that catatonia mainly belongs to schizophrenia doesn’t hold up anymore.
Newer research shows it appears more often in mood disorders like depression or bipolar disorder, and it can also show up with neurological illnesses or medication reactions.
A meta-analysis of 74 studies (over 100,000 patients) found a pooled average prevalence of ~9.2%, but prevalence varied widely across settings and patient populations, indicating that catatonia remains comparatively common among acute psychiatric and medical inpatients.
According to Max Fink, M.D., one of the most influential researchers on catatonia, the condition is often missed because clinicians mistakenly fold its symptoms into broader diagnoses like depression or psychosis.
He emphasizes that catatonia should be recognized as a distinct treatable syndrome, because when accurately identified and managed with appropriate interventions, many patients show rapid improvement. In other words, recognizing catatonia early is not just clinically useful; it can be critical for patient recovery.
Read More: Mental Health Matters: How to Foster Open Conversations in Your Family
Signs and Symptoms: How Catatonia Can Present
Catatonia isn’t one uniform presentation. One person may remain motionless for hours. Another may pace restlessly or mimic movements. This wide range of possible behaviors often contributes to missed diagnoses.
According to DSM-5 diagnostic guidelines, a person must show at least 3 of 12 core symptoms.
These include:
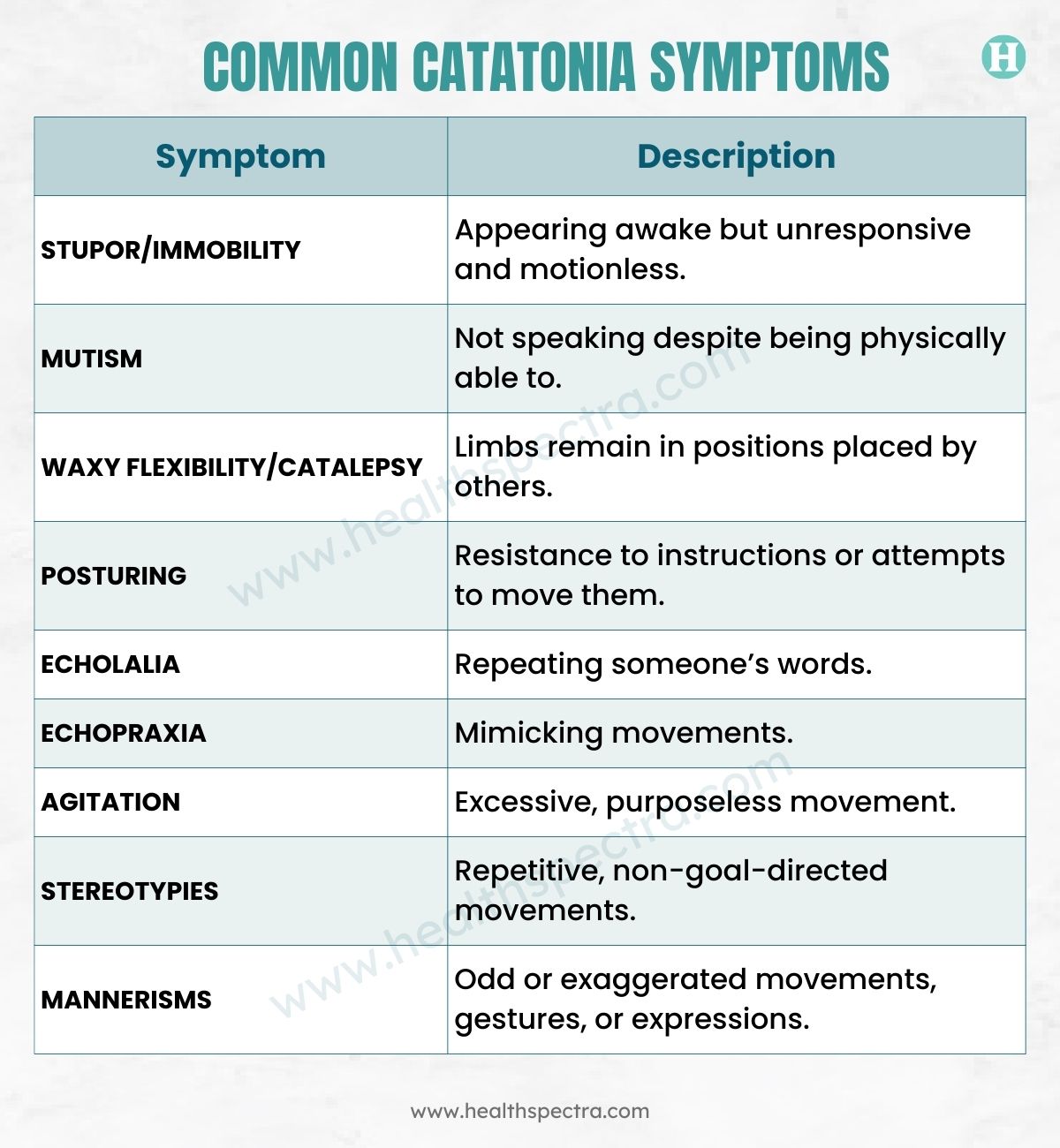
Even though pop culture focuses on immobility, psychiatrists emphasize that catatonia can present with severe agitation, known as the excited or hyperkinetic form.
Types of Catatonia
Catatonia doesn’t show up in just one way. It exists on a spectrum, and understanding these patterns helps clinicians judge urgency, identify risks, and choose the right treatment. The three major types are retarded, excited, and malignant catatonia, each with its own signature signs.
1. Retarded (Akinetic) Catatonia
This is the form most people recognize. Movement slows dramatically or stops altogether. The person may seem awake but emotionally distant, often sitting or standing in one position for long stretches. Because it looks calm, it’s easy to underestimate, yet it can severely impair daily functioning.
Key features:
- Marked slowing or immobility.
- Minimal or absent speech.
- Waxy flexibility or rigid posturing.
- Staring and withdrawal from the environment.
2. Excited Catatonia
Here, the problem isn’t stillness but overstimulation. The person becomes restless, agitated, or impulsive, sometimes mimicking others’ words or gestures. It’s frequently confused with mania or delirium unless someone identifies the catatonic motor patterns beneath the behavior.
Common signs:
- Constant pacing or agitation.
- Repetitive or purposeless movements.
- Echolalia (repeating words) or echopraxia (mimicking movements).
- Sudden switches between agitation and quietness.
3. Malignant Catatonia
This is a medical emergency. Along with catatonic symptoms, the body’s temperature, blood pressure, and heart rate start to destabilize. Without rapid intervention, the condition can escalate quickly and become life-threatening.
Red-flag symptoms:
- High fever with rigidity.
- Rapid or unstable heart rate.
- Blood pressure fluctuations.
- Confusion or altered consciousness.
According to Stephan Heckers, MD, M.Sc., catatonia is a heterogeneous psychomotor syndrome: in some patients, it presents as immobility and mutism, while in others it appears as agitation or hyperactivity.
Read More: Paranoid Personality Disorder: Understanding Causes, Symptoms, and Treatment
Why Catatonia Happens: Common Causes and Risk Factors

Catatonia rarely appears on its own. It’s usually the brain’s response to intense psychiatric stress, medical illness, or neurological disruption. Think of it as a final common pathway where multiple conditions can push the nervous system into dysregulation. Understanding the underlying cause is essential because treatment depends heavily on what triggered it.
Psychiatric Causes
Mood disorders sit at the top of the list. Severe depression and bipolar disorder, especially mixed or depressive episodes, are the most frequent psychiatric settings for catatonia.
Psychotic disorders can also trigger it, but less often than people assume. A more recent meta-analysis of clinical samples reports overall catatonia prevalence across psychiatric illnesses, not specifically that mood-episode prevalence exceeds schizophrenia-episode prevalence.
Common psychiatric triggers:
- Major depressive episodes
- Bipolar disorder
- Psychotic illnesses
Neurological and Medical Conditions
When catatonia shows up outside psychiatry, it often stems from serious disruptions in brain or body regulation. Autoimmune diseases like anti-NMDA receptor encephalitis, seizures, metabolic imbalances, head trauma, or overwhelming infections can all lead to catatonic symptoms. These cases are easy to miss because medical teams may focus primarily on the physical illness.
Medical and neurological triggers include:
- Autoimmune encephalitis
- Epilepsy
- Traumatic brain injury
- Metabolic derangements
- Severe systemic infections
Read More: 16 Natural Treatments for Bipolar Disorder – Know The Ways!
Medication or Substance-Related Causes
Sometimes the problem comes from what a person is taking, or suddenly stops taking. Abrupt benzodiazepine withdrawal, adverse reactions to antipsychotics, certain medical drugs like corticosteroids, or intoxicating substances can all push the nervous system into a catatonic state.
Potential triggers:
- Benzodiazepine withdrawal
- Antipsychotic reactions
- Steroids and other medical drugs
- Substance intoxication
Underlying Neurobiology
The most widely accepted theories point to disrupted neurotransmitter systems. Reduced GABA activity, dopamine pathway dysfunction, and changes in glutamate/NMDA signaling all interfere with the brain’s ability to initiate movement and regulate responsiveness. These pathways explain why benzodiazepines, which boost GABA, often lead to rapid improvement.
Key mechanisms involved:
- GABA dysfunction
- Dopamine disruption
- Glutamate/NMDA receptor alterations
When these systems misfire, the brain loses its usual balance between initiation and inhibition. That’s when catatonia emerges, and why identifying the root cause matters just as much as treating the symptoms.
Diagnosis: How Catatonia Is Detected
Catatonia is diagnosed clinically, meaning no single lab test or scan can confirm it. Instead, clinicians rely on observation and structured assessments.
1. DSM-5 Diagnostic Criteria
A person must show three or more of twelve psychomotor signs, including immobility, mutism, posturing, agitation, and echo phenomena.
2. Bush–Francis Catatonia Rating Scale (BFCRS)
Widely used in hospitals to:
- Identify catatonia
- Track severity
- Guide treatment response
The BFCRS includes both screening signs and extended evaluation items.
3. Rule-Out Evaluations
Because catatonia overlaps with:
- Severe depression
- Delirium
- Dementia
- Seizure activity
- Neuroleptic malignant syndrome
Clinicians must carefully exclude these possibilities. Early recognition matters because untreated catatonia can deteriorate quickly, especially if the patient stops eating or drinking.
Treatment Approaches: What Actually Works

Catatonia responds impressively well to the right treatment, especially when it’s caught early. Many patients improve within hours or days, which is why timely intervention matters.
- First-Line Treatment: Benzodiazepines: Lorazepam is the go-to option because it boosts GABA, the neurotransmitter most closely linked to catatonic symptoms. Clinicians often start with a lorazepam challenge, 1–2 mg, and watch for rapid improvement. If symptoms ease within minutes to hours, it strongly supports the diagnosis.
- Electroconvulsive Therapy (ECT): When benzodiazepines aren’t enough or when the case is severe, ECT steps in. It’s fast, safe, and often life-saving, particularly for malignant catatonia. The American Psychiatric Association reports remission rates above 80 percent, making ECT one of the most effective interventions in psychiatry.
- Treating the Underlying Cause: Catatonia is almost always triggered by something else, so stabilizing the root problem is essential, whether that’s depression, bipolar disorder, an infection, an autoimmune condition, or a medication reaction. Without this step, symptoms may return even after initial improvement.
- Supportive Care: Because movement and responsiveness can be limited, patients need solid medical support: hydration, proper nutrition, clot-prevention, skin protection, and monitoring for complications. These simple measures prevent serious problems like muscle breakdown, dehydration, or aspiration.
Prognosis and What To Know: Recovery, Risks, and Misconceptions
Most people recover well from catatonia when it’s recognized early and treated correctly. The speed of response can be striking, which is why timely diagnosis is the biggest factor shaping long-term outcomes.
Why Prognosis Is Usually Good
- Benzodiazepines are readily available and work quickly.
- ECT has excellent success rates for resistant or severe cases.
- Many underlying triggers, mood disorders, infections, and medication reactions are treatable.
- Catatonia rarely persists once the root cause is addressed.
Complications if Untreated
- Dehydration and severe malnutrition
- Pressure sores from immobility
- Blood clots and pulmonary embolism
- Autonomic instability, especially in malignant catatonia
These complications can escalate fast, which is why catatonia should never be managed with a wait-and-watch attitude.
Common Misconceptions
- It only occurs in schizophrenia. Mood disorders, major depression, and bipolar disorder are more common triggers.
- It always looks like stillness. There’s also excited catatonia, marked by agitation and constant movement.
- It’s rare. Research suggests it’s underrecognized and not uncommon.
- It resolves on its own. Left untreated, catatonia can become dangerous or life-threatening.
When To Seek Help: Red Flags and Urgent Signs
Catatonia can go from concerning to dangerous faster than most people expect. The key is not to second-guess what you’re seeing. If someone suddenly shifts into behaviors that feel disconnected from their usual self, it’s better to act early rather than wait for things to settle on their own. Catatonia is treatable, but only if the person gets prompt medical attention.
Immediate Red Flags
Watch for these shifts, especially if they appear suddenly:
- Immobility or freezing in place with no clear reason.
- Not speaking or barely responding despite being awake.
- Holding unusual postures for long periods.
- A blank, disconnected expression, even when someone is right in front of them.
- Refusing food or water in a way that feels intentional rather than accidental.
- Echoing words, gestures, or movements (echolalia or echopraxia).
These signs don’t always feel dramatic, which is why families often overlook them. But together, they paint a picture that requires a quick medical evaluation.
Emergency Signs (Possible Malignant Catatonia)
Here’s where things move into true emergency territory. If any of the following appear, call emergency services immediately:
- High fever that comes out of nowhere.
- Dangerous changes in heart rate, unusually fast or slow.
- Sharp swings in blood pressure.
- Severe confusion or disorientation.
- Marked rigidity or near-total stiffness.
- Intense agitation or sudden aggression.
- Any behavior suggesting self-harm or danger to others.
Malignant catatonia is a medical emergency. Even a few hours of delay can lead to organ failure, blood clots, or life-threatening complications.
Conclusion
Catatonia sits at the crossroads of psychiatry and neurology, which is exactly why it slips past so many clinicians and families. It doesn’t always look dramatic. But once you know the patterns, the picture becomes clearer, and the condition becomes far easier to spot before it spirals.
The encouraging part is that catatonia is one of the most treatable acute psychiatric syndromes we have. When recognized early, many people respond quickly to benzodiazepines, and those who don’t often improve with ECT. Recovery can begin within days, sometimes even hours. The real danger isn’t the condition itself, it’s the delay in identifying it.
Better training, better screening, and more open conversations can prevent the complications that turn catatonia into a medical emergency. Families, clinicians, and caregivers all play a role in noticing those early signs and acting on them.
In the end, understanding what catatonia is, why it emerges, and how treatment works lays the foundation for faster diagnosis and safer outcomes.
FAQs
What is catatonia in simple terms?
Catatonia is a state where a person’s movement, speech, and responsiveness shift in extreme ways. They might become unusually still or stop talking altogether. Some people hold the same posture for long periods, while others repeat odd movements.
The mind feels stuck, even though the person may look awake. It’s essentially a disruption in how the brain controls behavior and motor activity.
Is catatonia dangerous?
It can turn dangerous if it isn’t recognized early. People may stop eating or drinking, which leads to dehydration and medical instability. In malignant catatonia, the body’s temperature, blood pressure, and heart rate can swing unpredictably. Without urgent care, these changes can become life-threatening. With fast treatment, though, the risks drop dramatically.
How is catatonia diagnosed?
Clinicians watch for specific psychomotor signs, such as mutism, immobility, posturing, or agitation. A diagnosis usually requires at least three out of twelve key symptoms. Many hospitals use the Bush–Francis Catatonia Rating Scale to measure severity.
Doctors also rule out medical issues that can mimic catatonia. The goal is to identify the condition early, so treatment can begin right away.
What is the first-line treatment for catatonia?
Benzodiazepines, especially lorazepam, are the first and most effective initial treatment. Many people show improvement within hours of the first dose. If symptoms don’t respond or the condition is severe, ECT becomes the next recommended option. It has a strong track record of rapid recovery. Early treatment often prevents complications and speeds up healing.
Can catatonia happen with depression or bipolar disorder?
Yes, mood disorders are actually the leading causes of catatonia. Severe depression and bipolar episodes can disrupt brain circuits that govern movement and behavior. This is why a person may suddenly become silent, rigid, or agitated during a mood shift.
Catatonia is not limited to psychotic disorders. Recognizing this link helps clinicians treat the root condition more effectively.
Does catatonia mean someone is unconscious?
No, most people with catatonia are awake and aware of their surroundings. They simply can’t initiate movement, speech, or responses the way they normally would. It can look like unresponsiveness, but it isn’t the same as being unconscious. Their mind may feel locked in while the body stays still. This is part of why catatonia is so often misunderstood.
References
- Cleveland Clinic. (n.d.). Catatonia
- StatPearls. (2023, May 8). Catatonia
- WebMD. (n.d.). What is catatonia?
- Medscape. (n.d.). Catatonia: Overview
- Osmosis. (n.d.). Catatonia
- Kahl, K. G., & Baghai, T. C. (2024). Catatonia in psychiatric practice: Current perspectives. The Lancet Psychiatry, S1470‑2118(24)04607‑4
- Apollo Hospitals. (n.d.). Catatonia: Causes, symptoms, and treatment
- Wilson, J. E., Niu, K., & Heckers, S. (2025). Recent advances in understanding catatonia: Clinical and neurobiological perspectives. ScienceDirect
- Fink, M., & Taylor, M. A. (2014). Catatonia: Diagnosis and management. PMC
- Royal College of Psychiatrists. (n.d.). Catatonia
- MDPI. (2023). Catatonia: Clinical features and treatment strategies. Clinics and Practice, 13(4), 57
- Robinson, L. (2023). Methylphenidate treats catatonia in schizophrenia
In this Article

