

")





")

")

")



Frequent headaches are often dismissed as just an inconvenience, caused by a hectic schedule, poor diet, or general exhaustion. But when these headaches start coming with uncomfortable regularity, and their character gradually changes from normal pressure to a more insistent, sensory-disturbing pain, it usually deserves closer attention. A surprisingly large number of individuals continue calling these episodes “simple headaches,” even when the pattern has clearly evolved.
Chronic migraine is one such condition that quietly develops behind the façade of ordinary discomfort. Defined by its persistent frequency and its neurological (brain-related) signature, it affects daily functioning far more deeply than people assume. Recognising this early is important because timely intervention can stop the progression toward disability.
This article examines chronic migraine with a slightly broader lens – not only the usual clinical criteria, but also the subtler indicators, the overlooked risks, and the treatment advances that are now reshaping how neurologists manage long-standing headache disorders.
Key Takeaways – What You’ll Learn
By the end of this article, you’ll understand:
- What chronic migraine really means and how it differs from the usual types of headache.
- Subtle early warning signs that your recurring headaches may actually be evolving into something chronic.
- What triggers worsen migraine, and which risk factors can you control.
- Modern treatment options – from medications to lifestyle changes – that genuinely help.
What Is a Chronic Migraine?
Chronic migraine is diagnosed when someone has 15 or more headache days each month, and at least 8 of those days behave like a migraine – meaning the pain may throb or pulsate, feel one-sided, or come with nausea and sensitivity to light or sound.
This definition may appear straightforward, but it reflects a major shift in how the brain functions.
Unlike episodic migraine, which comes and goes, chronic migraine creates an almost constant state of vulnerability. The nervous system is in a heightened state most of the time – a condition researchers describe as “neural hyperexcitability.”
Key pain pathways – especially the trigeminal nerve (the major pain nerve) and chemicals such as CGRP (Calcitonin Gene-Related Peptide – a migraine pain chemical) – remain sensitised, which means even small disturbances can trigger an attack.
Many patients do not realise that chronic migraine is not a psychological or stress-based issue but a neurological disturbance with measurable physiological changes. Imaging and neurochemical research consistently show altered pain processing, cortical sensitivity (sensitive brain surface), and inflammation around nerve terminals.
How Chronic Migraine Differs from “Regular” Headaches
Many people assume all headaches fall into the same category. Not true. The distinctions are clearer when placed side by side:
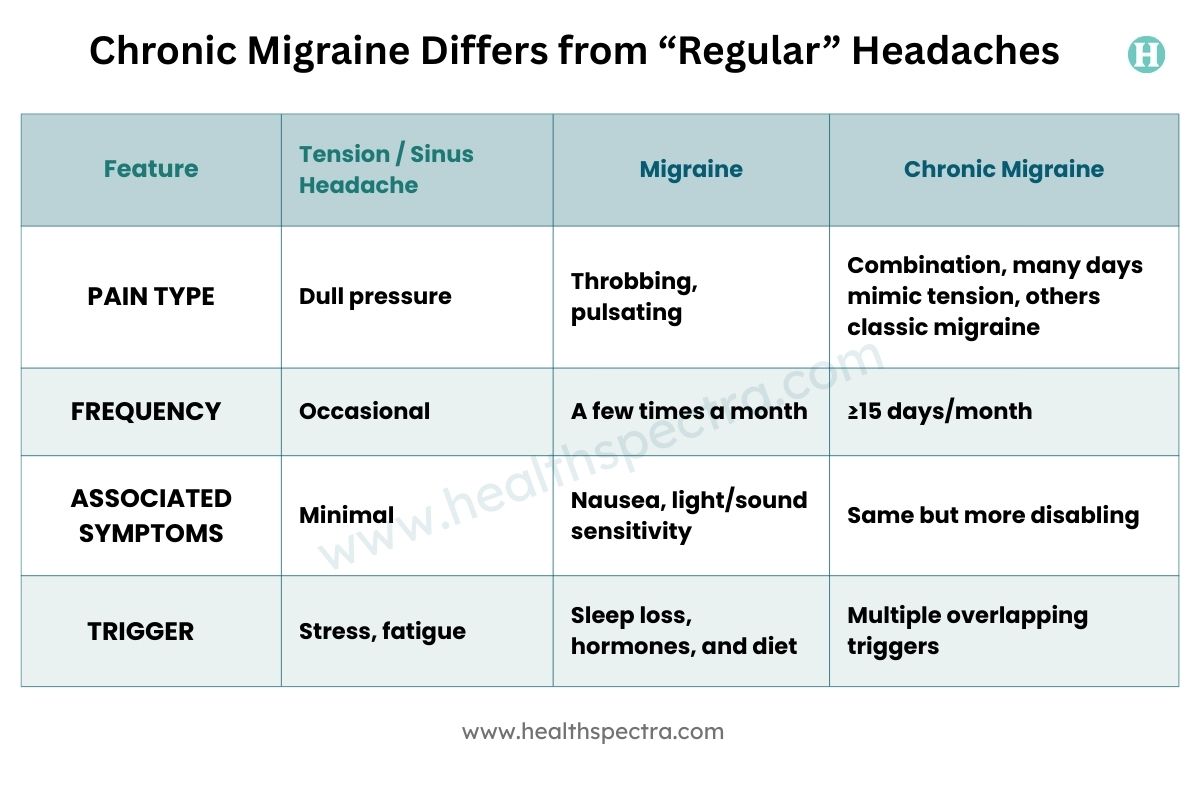
A common mistake neurologists see is people calling their recurring migraine sinus headaches. Studies show most “sinus headaches” are actually migraine with nasal symptoms like congestion or watery eyes.
Common Triggers and Risk Factors

Migraine are highly individual. The same trigger that causes a severe attack in one person may not affect someone else at all. But still, certain patterns are well recognised.
1. Lifestyle and Environmental Instability
A migraine brain is highly reactive to sudden changes. So things like:
- irregular sleep (too little OR too much)
- skipped meals
- dehydration
- long screen-hours
- bright or flickering lights
- too much caffeine or sudden caffeine withdrawal
- loud noise or strong odours
…can easily trigger episodes.
2. Hormonal Changes
Migraine in many women gets worse around menstruation because of the fluctuations in estrogen (female hormone). Pregnancy, perimenopause, and hormonal contraception also play a role. Hormones don’t cause migraine, but they make the brain far more reactive.
3. Dietary Links
Not everyone gets food-triggered migraine, but some well-studied triggers include:
- Red wine
- Aged cheese
- Processed meats containing nitrates
- Artificial sweeteners
- Fasting or delayed meals
These do not cause migraine by themselves, but they provoke an already vulnerable system.
4. Medical and Genetic Factors
You may have a higher risk if you have:
- A family history of migraine
- Anxiety disorders, depression, or sleep problems
- Obesity, which increases inflammation
- Medication overuse – especially OTC painkillers
Rebound headache due to frequent painkiller use is one of the most underrated causes of chronic migraine.
Early Signs That Mild Headaches May Be Chronic Migraine

Chronic migraine doesn’t appear suddenly. It develops slowly, and these are the early signs:
- Headaches that gradually increase in frequency over months.
- Pain that often begins around the temples or behind the eyes.
- Light or sound sensitivity becomes more noticeable with time.
- A sense of mental fog, irritability, or unusual fatigue appears before or after attacks.
- Painkillers become frequent, more than two or three times a week.
- The person starts skipping work or cancelling plans as the pain becomes too frequent.
Ignoring these signs is what often allows episodic migraine to convert into chronic migraine.
Read More: Exertion Headaches: Why Your Workout Might Trigger Head Pain & What to Do About…
Diagnosis – How Doctors Confirm Chronic Migraine
Most diagnoses are made clinically, according to the International Headache Society guidelines. A neurologist will ask you about:
- How many days do you get a headache per month
- What the pain feels like
- Whether you get nausea, aura (sensory warning), or sensitivity to light/sound
- Your medication history
- Possible triggers
A headache diary helps tremendously by revealing patterns you may not notice.
Scans (MRI or CT) are only to rule out other conditions such as tumours, aneurysms, or sinus disease. They don’t diagnose migraine.
Read More: Tackle Tension Headaches: 5 Tension-Relief Devices for Stress-Free Living
Treatment Options – From Relief to Prevention

Chronic migraine needs a two-way approach:
(1) Treating attacks when they come, and
(2) Preventing future attacks.
Both are equally important.
1. Acute (Abortive) Treatments
Used before an attack begins, these medicines also aim to stop the progression.
- Triptans (sumatriptan, rizatriptan)
Work by blocking pain pathways. Most effective when taken early. - NSAIDs and paracetamol
Only for mild episodes, but excessive use worsens long-term outcomes. - CGRP receptor antagonists (ubrogepant, rimegepant)
Important newer options. Works without causing rebound headaches. - Lasmiditan
Works differently and is safer in people who cannot take triptans due to heart disease.
2. Preventive (Prophylactic) Therapies
Preventive therapy aims to reduce the number of monthly migraine days. It is essential for chronic migraine.
- Beta-blockers (heart/calming drugs) like propranolol
- Antiepileptic drugs (seizure medicines) like topiramate
- Antidepressants, including amitriptyline (helps with sleep too)
CGRP Monoclonal Antibodies
This is one of the biggest modern advances. These monthly injections (erenumab, fremanezumab, galcanezumab) target specific pain-related pathways and are especially beneficial in chronic migraine. Many patients report a substantial reduction in attack frequency.
OnabotulinumtoxinA (Botox®)
OnabotulinumtoxinA is approved specifically for individuals with 15 or more headache days per month. Injections are taken once every 12 weeks. Many patients see major improvement.
Preventive therapies need consistent use for at least 2–3 months before reliable improvement appears.
3. Non-Drug and Adjunctive Strategies
Several non-pharmacological approaches have supportive evidence:
- Biofeedback (body-awareness training) and relaxation training
- Cognitive Behavioral Therapy for stress-related patterns
- Yoga or low-impact aerobic activity
- Acupuncture for reducing frequency
- FDA-approved neuromodulation devices (nerve-calming gadgets), as advised by Jason Sico, a neurologist, can also help. For example: Cefaly® and gammaCore®
These therapies help stabilise the nervous system and complement medical treatment.
Managing Chronic Migraine in Daily Life
Chronic migraine needs daily management – not just treatment during pain episodes. Certain routines help reduce neural instability:
- Maintain uniform sleep and meal timings.
- Keep hydration steady.
- Limit caffeine without abrupt withdrawal.
- Minimise long screen exposure without breaks.
- Use soft or indirect lighting when possible.
- Create a calmer work environment with ergonomic posture (body-friendly posture).
- Avoid habitual reliance on painkillers.
- Track symptoms in a structured diary.
Education for family members or colleagues is also useful, as migraine impairment is often invisible.
Read More: Losing Weight Can Help Reduce Obesity Induced Migraine Headaches
When to Consult a Neurologist

Seek a specialist’s evaluation when:
- Headaches occur more than 10–15 days per month
- Pain worsens despite using OTC medicines
- You have visual aura, numbness, or speech difficulty
- Headaches get triggered by coughing, exertion, or sudden posture change
- You suspect medication-overuse headache
Early consultation prevents chronicity and helps avoid medication-overuse patterns. As Dr. Nancy L. Mueller, a neurologist, puts it, the better you understand how your headache begins, the sooner you can calm it.
Read More: How to Treat Headaches Behind The Eyes
Final Thoughts
Chronic migraine is difficult, but it becomes manageable after the pattern is recognised and when it is treated with some structured plans. Many patients improve when preventive therapy is used consistently and trigger-stabilising habits are maintained. Even small corrections – reducing painkiller overuse, keeping regular sleep, adjusting routine – can shift the course of the condition. With proper guidance, the disease becomes far less disruptive than people expect.
Quick Recap
- Chronic migraine is a neurological disorder with defined diagnostic boundaries.
- It differs substantially from ordinary headaches in frequency, neurological features, and long-term impact.
- Modern treatment includes CGRP-based therapies, Botox®, and precise preventive medications.
- Timely intervention and stable habits help control progression.
FAQs
1. Are repeated mild headaches always migraine?
No. However, persistent frequency with sensory sensitivity often signals migraine rather than tension headache.
2. Do chronic migraines ever reverse?
It is not “curable,” but it is very treatable. Many people see major improvement with consistent preventive therapy.
3. Are CGRP inhibitors safe for long-term use?
Current evidence suggests good safety and tolerability – they target precise mechanisms without broad systemic impact.
4. Does diet alone control chronic migraine?
Diet supports stability, but chronic migraine generally requires medical preventive therapy.
5. How to confirm if my mild headache is really migraine?
If the headache is throbbing, worsens with activity, or is accompanied by nausea, sensitivity to light, or even sound, it is likely a migraine.
References
- Chronic migraine. (2025, July 3). Cleveland Clinic.
- Mungoven, T. J., Henderson, L. A., & Meylakh, N. (2021). Chronic Migraine Pathophysiology and Treatment: A Review of Current Perspectives. Frontiers in Pain Research, 2, 705276.
- Ruschel, M. a. P., & De Jesus, O. (2024, July 5). Migraine headache. StatPearls – NCBI Bookshelf.
- Silberstein, S. D., Calhoun, A. H., Lipton, R. B., Grosberg, B. M., Cady, R. K., Dorlas, S., Simmons, K. A., Mullin, C., Liebler, E. J., Goadsby, P. J., Saper, J. R., Calhoun, A. H., Cady, R. K., Dexter, J., Silberstein, S. D., Young, W., Marmura, M., Nahas-Geiger, S., Da Silva, A., . . . Eller, M. (2016). Chronic migraine headache prevention with noninvasive vagus nerve stimulation. Neurology, 87(5), 529–538.
- Wattiez, A., Sowers, L. P., & Russo, A. F. (2020). Calcitonin gene-related peptide (CGRP): role in migraine pathophysiology and therapeutic targeting. Expert Opinion on Therapeutic Targets, 24(2), 91–100.
- World Health Organization: WHO. (2025, October 24). Migraine and other headache disorders.
- Yuan, H., & Chuang, T. (2021). Update of neuromodulation in chronic migraine. Current Pain and Headache Reports, 25(11), 71.
In this Article