







")

")

")



Abortion is a medically safe and common procedure used to end a pregnancy, provided it’s done under qualified medical supervision. It’s part of essential reproductive healthcare and has been practiced safely for decades across the world.
There are two primary methods: medication abortion (often called “the abortion pill”) and surgical abortion (an in-clinic procedure). Both are highly effective when performed correctly and chosen based on the stage of pregnancy, personal preference, and medical factors.
Understanding the process can help you make a decision that feels right for you, both physically and emotionally. This article breaks down how each method works, what to expect before, during, and after the procedure, and how recovery and after-care differ.
It also explains the safety, effectiveness, and key considerations to keep in mind, so you can approach the decision with clarity, confidence, and accurate information rather than fear or misinformation.
What is a Medication Abortion?

Medication abortion uses a combination of drugs, typically Mifepristone followed by Misoprostol, to end a pregnancy. The mifepristone blocks progesterone (a hormone the pregnancy needs) and misoprostol prompts uterine contractions to expel the pregnancy contents.
According to Dr. Bela Ganatra, Head of the Preventing Unsafe Abortion Programme at the World Health Organization, “There is a large body of evidence on the safety and efficacy of medical abortion from all over the world. Mifepristone and misoprostol have been moved to the core Essential Medicines List, and the requirement for close medical supervision is removed.”
How it works
- The first pill (mifepristone) is taken under supervision; it halts the pregnancy.
- Then, usually 24–48 hours later, misoprostol is taken (or given), which causes uterine contractions and bleeding to complete the abortion.
- This process mimics a heavy period or miscarriage more than a surgical procedure.
- It can often be done at home or in a clinic/tele‑health setting, depending on the region and provider.
Time frame and situation
- Many protocols allow this up to about 10–12 weeks of gestation in most settings. Studies show effectiveness even in the late first trimester.
- Because it can be done at home (in some places), it offers additional privacy and flexibility.
What you should expect
- Cramping and bleeding (often heavier than a period).
- Passage of pregnancy tissue (with clots, sometimes).
- Side‑effects: nausea, fatigue, possibly chills, diarrhea, common but usually mild.
- Follow‑up is important to ensure the pregnancy is fully terminated and that no complications are present.
Effectiveness
- Data show that in early gestation (up to around 9–10 weeks), the success rate ranges from 95 % to98 %.
- For example, a US study found 6% success for medication abortion before 64 days vs 99.8% for surgical, but with slightly higher repeat procedure risk.
- A major review about the safety and effectiveness of first-trimester medication abortion concluded, “Medication abortion is extremely safe. Serious adverse events occur in less than one‑third of one percent.”
What is a Surgical Abortion?

Surgical abortion refers to in‑clinic procedures carried out by a trained provider to remove the pregnancy tissue. This can include vacuum aspiration (early pregnancy) or dilation and evacuation (D&E) for later stages.
Procedure type and duration
- For early gestation(first trimester), the procedure is typically vacuum/suction aspiration: takes about 5‑15 minutes under local or light sedation.
- For later gestation (after ~12 weeks), D&E is more common, which takes longer and may involve more preparation.
- Because it’s procedural, the provider ensures the pregnancy tissue is removed and often checks completion immediately.
Time frame and situation
- Surgical abortion is commonly used when the pregnancy is beyond the window for medication abortion, or if the medication route isn’t suitable (medical conditions, patient preference).
- Many clinics report higher effectiveness and fewer follow‑ups needed. It can require fewer appointments. The procedure takes a short amount of time. It is more effective; patients usually do not have heavy bleeding at home.
What to expect
- You’ll go to a clinic/hospital for the procedure.
- After the procedure, you’ll be observed for a short time (maybe hours) before going home.
- Some cramping and light bleeding afterward is normal.
- Because the tissue is removed in the clinic, the “bleeding and passing clots at home” phase is typically shorter than for medication abortion.
Effectiveness
- Success rates are very high, often around 98% or better for first‑trimester surgical abortion.
- Complication rates are low; for first‑trimester procedures in otherwise healthy people, risks are minimal.
Comparing Medication and Surgical Abortion: Key Differences
Let’s break down how they differ across several key aspects:
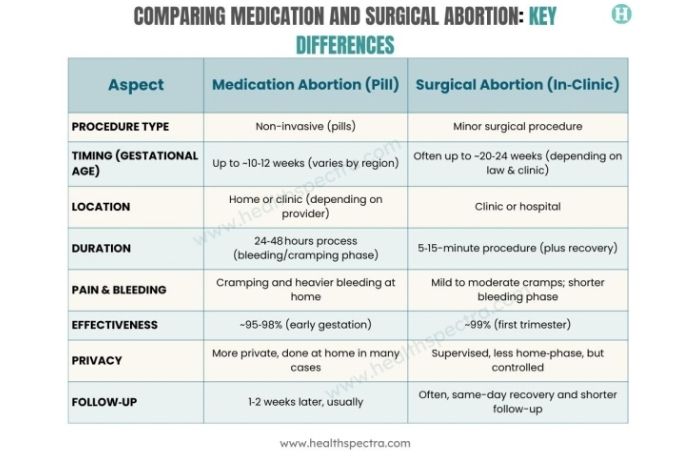 This comparison illustrates that each method has trade-offs. What this really means is that one isn’t universally “better”; it’s about what fits your situation, timeline, preferences, and health.
This comparison illustrates that each method has trade-offs. What this really means is that one isn’t universally “better”; it’s about what fits your situation, timeline, preferences, and health.
How to Choose the Right Option for You
Here are key factors to help you decide.
1. Gestational age
How far along you are is one of the strongest deciding factors. Medication abortion is generally recommended up to about 10‑12 weeks (varies by local guideline). Beyond that, surgical options may be the only recommended route.
2. Access to care
- If you live in a region with limited clinic access, medication abortion (especially via telehealth) may offer increased flexibility.
- If you prefer being under direct provider care with less “at‑home passing” time, surgery might feel more secure.
3. Personal preference and comfort
Your comfort with how the process unfolds matters:
- Do you prefer to manage things at home, privately, with minimal clinic visits? Medication may appeal.
- Do you prefer coming to the clinic once and getting the process done under supervision? Surgery may appeal.
4. Medical conditions
Certain health conditions may make one method more or less appropriate (for example, certain bleeding disorders, an IUD in place, or anemia). Always consult a qualified provider.
5. What do you feel ready for emotionally and physically
Recovery time, what happens at home, how you feel about bleeding and passing tissue at home vs the clinic, these matter. What you prefer in terms of privacy, number of visits, and follow‑up care should factor in.
6. Legal/regional policy
In your country or region, one method may be more widely available than the other. Regulations on telehealth, home provision, and gestational age limits may shape your options.
Bottom line: Both methods are safe and effective when done under professional care. Which is “right” depends on you. Best step: talk with a licensed provider who can walk you through your specific situation, health history, timeline, and preferences.
Safety, Side Effects, and Possible Risks

It’s important to know what’s common, what’s rare, and when to seek help.
Common side effects (both methods)
- Cramping, bleeding (heavier than a period for some)
- Fatigue, nausea, sometimes fever/chills (especially with medication)
- Emotional reactions: relief, sadness, unexpected feelings, and normal.
Rare complications
- An incomplete abortion (some tissue remains) may require follow‑up. Study: In the late first trimester, medical abortion had ongoing pregnancy rates slightly higher than surgical.
- Heavy bleeding requiring medical attention (rare). For medication abortion in the U.S., serious adverse events requiring hospitalization are <0.3%.
- Infection (rare)
- With surgical methods, there is a small risk of uterine perforation and cervical injury, but very uncommon in experienced hands.
- For later‐gestation surgical abortions, complication rates are somewhat higher than first trimester.
According to a review, medical methods are safe, effective, simpler, and potentially allow greater privacy, while no difference in safety has been found between surgical and medical abortions when performed by qualified providers, indicating that both are safe and effective options that should be offered equally.
Read More: Can You Still Get Pregnant After an Abortion? What Doctors Want You to Know
Recovery and Aftercare Tips

Recovery after an abortion is usually straightforward, but giving your body and mind the right care makes a real difference. Most people recover quickly, yet it’s normal to feel tired, crampy, or emotionally sensitive for a few days.
Proper rest, hydration, and gentle self-care help your body return to balance, while knowing what’s normal and what’s not can prevent unnecessary worry. This section walks you through simple, evidence-based aftercare tips for both medication and surgical abortions, including physical recovery, emotional well-being, and signs that call for medical attention.
Here’s what you should know about aftercare and recovery for both methods.
Rest and self‑care
- Ensure you have a quiet day or two post‑procedure or post‑medication when bleeding/cramping is at its peak.
- Use a heating pad for cramps. Over‑the‑counter pain relief (ibuprofen) usually works; confirm with your provider.
- Stay hydrated.
- Eat nourishing food. Your body just went through a process.
Physical restrictions
- Avoid strenuous exercise or heavy lifting for at least 24–48 hours, or longer if your provider recommends.
- Avoid sexual intercourse until your provider gives the go‑ahead (often once bleeding reduces or stops and any recommended follow‑up is done).
- Use sanitary pads (not tampons) unless your provider says otherwise, because tampons may increase infection risk while bleeding continues.
Emotional after‑care
- It’s normal to have emotional reactions, relief, sadness, guilt, or mixed feelings.
- Talk with a trusted friend or partner if you feel comfortable.
- If you’re having strong distress, anxiety, or symptoms of depression, it’s okay to reach out to counseling or support services.
- You’re not “supposed” to feel a specific way. What matters is that you feel supported.
When to call a doctor
- High fever (above 38°C/100.4°F) lasting more than 24 hours.
- Bleeding that soaks more than two maxi pads per hour for more than two hours.
- Large clots (the size of an orange or bigger) or passing something that worries you (always good to ask).
- Foul‑smelling discharge (could signal infection).
- Severe pain not relieved by recommended medications.
- If your follow‑up shows pregnancy continues (ongoing pregnancy) or you’re concerned you may be pregnant again too soon.
Read More: Post-Abortion Anxiety and Depression: What’s Normal and When to Seek Help
Legal and Access Considerations

Access to abortion care isn’t the same everywhere; it’s shaped by local laws, healthcare systems, and social attitudes. Understanding the legal landscape where you live is essential before making any decision.
Regulations can vary by country, state, or even district, covering factors such as how far along a pregnancy can be, which methods are allowed, and whether telehealth services are permitted.
This section outlines the key legal and access considerations to keep in mind: how to find safe, verified providers; what the law says about home-based medication abortion; and where to turn for trustworthy information and support. Knowing your rights and the resources available to you helps ensure that any decision you make is both informed and safe.
- Laws around abortion vary greatly by country and region, gestational age limits, method availability, and telehealth restrictions.
- Home use of medication abortion is expanding in many regions, but you still need safe access to follow‑up and emergency care. For example, home‑based medication abortion showed success rates of ~95% in one review.
- Use verified clinics or licensed telemedicine providers only.
- Organizations like the World Health Organization (WHO), Planned Parenthood, and Marie Stopes International provide guidance and resources.
- Know your rights and local laws: whether abortion is legal in your region, under what conditions, and what providers are available.
Key Takeaway
Both medication and surgical abortion are safe, effective, and medically approved methods for ending a pregnancy when performed under proper medical supervision. Each comes with its own advantages, timing requirements, and recovery experiences, so the best choice isn’t about which is “better” in general; it’s about which is right for you.
Medication abortion offers privacy and a more natural process that can often be managed at home within the first 10–12 weeks of pregnancy. Surgical abortion, on the other hand, is faster, typically completed in one clinic visit, and may be more suitable later in pregnancy or for those who prefer a more controlled medical setting.
What matters most is that you make an informed decision in consultation with a qualified healthcare provider. Discuss your medical history, emotional comfort, and access to support during recovery. Ask every question you need to feel confident. When handled with proper guidance and care, both methods are safe and can be part of a responsible, supported choice for your health and well-being.
Frequently Asked Questions (FAQs)
Is the abortion pill safe to take at home?
Yes, for eligible candidates and under provider guidance, medication abortion is safe. Serious adverse events are very rare (<0.5%) in studies. But you must have access to follow‑up care and know when to seek help.
How painful is a surgical abortion?
Pain is usually mild to moderate and short‑lived with appropriate pain management. Most clinics use local anesthesia or light sedation, and the procedure is brief. Many people recover quickly.
Can I choose which method I prefer?
In many cases, yes, you can discuss with your provider which option you prefer, given your gestational age, health, and access. But in some regions, laws or clinical guidelines may steer you toward one or the other.
How soon can I return to normal activities after an abortion?
It depends on the method and how you feel. Often, you can resume light activity within 24‑48 hours, but avoid heavy exercise, sexual intercourse, or heavy lifting until your provider confirms it’s safe.
Does abortion affect future fertility?
No, when done safely and properly, neither medication nor surgical abortion is shown to affect future fertility. The risk of serious complications (which might affect fertility) is extremely low in healthy individuals.
References
- https://my.clevelandclinic.org/health/treatments/21899-medical-abortion
- https://en.wikipedia.org/wiki/Medical_abortion
- https://www.plannedparenthood.org/learn/abortion/the-abortion-pill
- https://www.aamc.org/news/what-medication-abortion-your-questions-answered
- https://www.acog.org/clinical/clinical-guidance/practice-bulletin/articles/2020/10/medication-abortion-up-to-70-days-of-gestation
- https://www.betterhealth.vic.gov.au/health/healthyliving/abortion-procedures-medication
- https://medlineplus.gov/ency/article/007382.htm
- https://www.ucsfhealth.org/treatments/medical-abortion
- https://www.bpas.org/abortion-care/abortion-treatments/the-abortion-pill/
- https://www.betterhealth.vic.gov.au/health/healthyliving/abortion-procedures-surgical
- https://www.ucsfhealth.org/treatments/surgical-abortion-first-trimester
- https://www.bpas.org/abortion-care/abortion-treatments/surgical-abortion/
- https://www.uclahealth.org/medical-services/obgyn/family-planning/patient-resources/surgical-abortion-first-trimester
- https://www.plannedparenthood.org/learn/abortion/in-clinic-abortion-procedures
- https://www2.hse.ie/conditions/abortion/methods/surgical/
- https://www.nhs.uk/tests-and-treatments/abortion/what-happens/
- https://www.nhsinform.scot/tests-and-treatments/non-surgical-procedures/abortion/types-of-abortion/
- https://www.ucsfhealth.org/treatments/surgical-abortion-second-trimester
In this Article